
Ian Ashdown, P. Eng., FIES, Senior Scientist, SunTracker Technologies Ltd.
Published: 2014/11/05
As a professional lighting designer, you will likely have read about the “blue light hazard” associated with white light-emitting diodes. You will have seen warnings like this (Willmorth 2014a):
“… long term exposure to blue light at 441nm caused lesions on the retinas of rhesus monkeys,”
and recommendations like this from the same author:
“Use the lowest CCT LED color with the highest CRI available to suit the lighting application – including avoidance of high CCT (> 5000K), low CRI (<80) sources altogether, and eliminate use of blue-light rich products, such as those generating >5500K at <65CRI.”
and even this (Kitchel 2000):
“…all persons with vision problems should be removed from a light environment where the predominant light waves are a temperature above 3500K or a wavelength less than approximately 500 nm.”
It is a confusing situation for lighting designers, as there are well-documented vision and health benefits to the use of high-CCT lighting. These benefits include circadian rhythm entrainment (e.g., Holzman 2010) and improved visibility (e.g., Berman et al. 2006). Taken together, the recommendations are at best contradictory.
As always, “… there is a need for more focused research leading to practical recommendations on this subject” (Willmorth 2014a). In the meantime however, lighting designers need to make informed decisions on behalf of their clients. What to do?
There is no short answer. As this article demonstrates, the issue of blue light causing retinal lesions is based on a misunderstanding of vision research work done in the 1970s. It is still an open question as to whether long-term chronic exposure to blue light may cause vision problems, but the evidence to date (known to this author at least) is not persuasive. [UPDATE 14/11/08 – see concluding paragraphs and SCENIHR (2012).]
[UPDATE 14/12/11 – See revised concluding paragraphs and GLA 2012.]
The recommendation above – “Use the lowest CCT LED color with the highest CRI available to suit the lighting application” – also highlights the danger to journalists when combining reviews of the academic literature with design recommendations. While it could be construed from the article that this recommendation is based on concerns about vision problems, it is instead advice that the author would communicate to any client (Willmorth 2014b), regardless of the academic literature.
To be perfectly clear, this article is in no way meant as a criticism of Willmorth (2014a). It is instead an exploration of how scientific research can be misinterpreted and then promulgated in good faith as scientific fact. It is a problem that all science journalists face, myself included.
More to the point however, this article attempts to clarify some of the issues concerning the “blue light hazard.” As lighting designers, it is important to realize that direct viewing of extremely high-brightness LEDs may cause eye damage. At the same time, it is important to understand that these concerns are distinct from everyday interior lighting design practices.
Background
Lighting Research Center researcher John Bullough published “The Blue-Light Hazard: A Review” in the Journal of the Illuminating Engineering Society (Bullough 2000), in which he summarized the research on the role of short-wavelength (i.e. deep blue) light and ultraviolet radiation in retinal damage. Quoting from this paper:
“For practical purposes with ‘white’ light sources, any condition resulting in direct exposure to luminances under 10,000 cd/m2 is unlikely to present a risk of photochemical injury to the retina. For such sources, calculation of the blue light hazard is not necessary.”
Putting this into context:
“… might lead one to believe [that] fluorescent lamps present greater risk than incandescent lamps, because they produce a greater portion of their light in the short-range portion of the visible spectrum. However, because fluorescent lamps also have low luminances (T12 lamps: 8,000 cd/m2; T8 lamps: 11,000 cd/m2; T5 lamps: 20,000 cd/m2), their potential risk for photochemical injury is negligible …”
Bullough examined potential risks in the context of medical equipment, industrial equipment, and high-flux theatrical lighting. In terms of extremely high-brightness LEDs, there is clearly a risk in viewing them directly. People with aphakia (absence of the lens of the eye, often due to surgical removal) may also be at risk. In general however, there is no blue light hazard for interior lighting applications.
Trust in Authority
So where did the current “blue light hazard” meme originate? Willmott (2014a) notwithstanding, why are lighting designers now being advised to avoid high-CCT lighting wherever and whenever possible?
The underlying problem is that lighting designers cannot be expected to follow the medical literature on which these recommendations may be based. How many people for example outside of the medical profession read such journals as Epidemiology and Biostatistics or Investigative Ophthamology & Visual Science? (How many people can even spell “ophthalmology” correctly, for that matter?)
The solution is beguilingly simple: trust in those who are experts in such matters. Lighting designers read trade journals such as Lighting Design & Application and Architectural SSL because of these publications’ reputation for accurate and useful information. Their technical articles are after all either written by qualified experts, or by staff writers who consult them.
Who we trust however is subject to the logical fallacy of argumentum ab auctoritate, or “argument from authority” (including trust in those who, like me, quote Latin phrases). In more colloquial terms, “Just because you say it’s so don’t make it so!”
To illustrate this argument, consider the quotation above (Willmorth 2014a):
“… long term exposure to blue light at 441nm caused lesions on the retinas of rhesus monkeys.”
The article in question is titled, “The Dark Side of BLUE LIGHT,” which was written by Kevin Willmorth, Consulting Editor for Architectural SSL. Educated at the University of Phoenix, he has over 33 years of experience in lighting design and product development. Given this, there is no reason to question his authority per se. However, we need to ask where this worrisome statement came from.
Like most trade journals, Architectural SSL has an aversion to publishing full references in its technical articles. There are two likely reasons for this: 1) very few readers will be interested in reading the referenced papers; and 2) full references consume valuable advertising space. Regardless of the reasons, the author can do no more than identify the name of the researcher and possibly the paper’s title in the text of the article.
In other words, trust in authority.
Full References
Thankfully, Willmorth was fairly specific in referencing (in the same sentence) “The Effects of Blue Light on Ocular Health (Kitchel, E. American Printing House for the Blind.” (The more common alternative is to simply say, “According to …”) A simple Web search leads directly to http://www.cclvi.org/contributions/effects1.htm. It is an online article, but it was originally published in the Journal of Visual Impairment and Blindness (Kitchel 2000).
Elaine Kitchel is Low Vision Project Leader at the American Printing House for the Blind, with a Masters of Education from the University of Arizona. In her review article, she writes:
“In an early study conducted by Ham, Ruffolo, Mueller and Guerry, (1980) rhesus monkeys were exposed to high-intensity blue light at 441nm for a duration of 1000 seconds. Two days later lesions were formed in the retinal pigmented epithelium (RPE.) These lesions consisted of an ‘inflammatory reaction accompanied with clumping of melanosomes and some macrophage invasion with engulfment of melanosomes which produce hypopigmentation of the RPE’ (Ham et al., 1980, p.1110).”
We now have a reference for the original quote, including a page number … or do we? Once again, the article does not include references, rather unhelpfully stating, “A bibliography is available separately.” Fourteen years after publication, it is unlikely that this unnamed document will still be available.
Trust in authority.
Monkey Business
Fortunately, it is possible with some effort to ascertain the proper reference. It is:
Ham, W. T., Jr., H. A. Mueller, J. J. Ruffolo Jr., and D. Guerry. 1980. “The Nature of Retinal Radiation Damage: Dependence on Wavelength, Power Level, and Exposure Time,” Vision Research 20(12):1105-1111.
William T. Ham and his fellow researchers were at the time associated with the Department of Biophysics, Virginia Commonwealth University (Richmond, VA). Vision Research being a highly respected peer-reviewed journal, their paper of course included copious references.
Trust in authority? Not quite … if you obtain and read the review paper, you will find no mention of “blue light at 441 nm” on page 1110. Here is what the authors wrote:
“Histological data, Ham et al., (1978), on the retina of the rhesus monkey demonstrate that short wavelength light plays a role in the clumping and phagocytosis of melanin. The appearance of a mild lesion in the RPE of the rhesus monkey at 90 days postexposure suggests a striking similarity to senile macular degeneration. In the opinion of the authors, long-term, chronic exposure to short wavelength light is a strong contributing factor to senile macular degeneration.”
This is an interesting observation that is apparently still valid – see for example Berman and Clear (2014) – but it is not what we are after.
In reading the full paper, there is an interesting figure caption on page 1107:
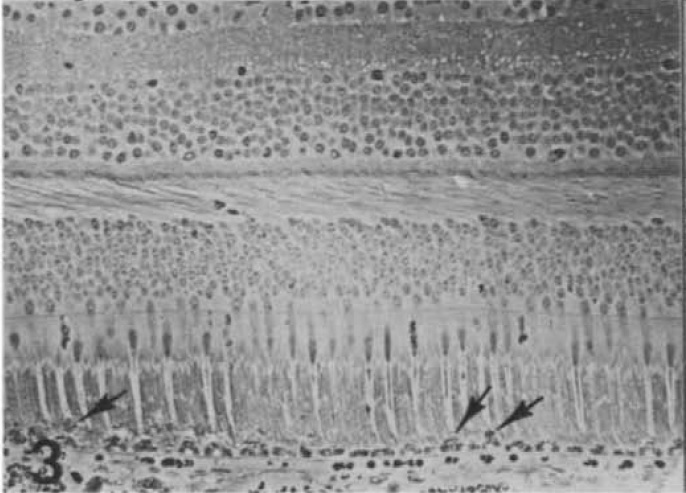
Fig. 3 – Retinal response in the same eye as Fig. 2 at 2 days after a 1000 sec exposure to 441 nm light (10 nm bandpass). The image diameter at the retina was 1 mm, and the radiant exposure was 33 J/cm2.
FIG. 1 – Retinal damage due to laser light exposure. (Source: Ham et. al. 1980.)
This microphotograph of a rhesus monkey’s retina is from research reported by Ham et al. (1978), which was based on an earlier paper (Ham et al. 1976), both listed in the references. The arrows in the image indicate the observed lesions.
It helps to have some appreciation of the nature of this research. Ten rhesus monkeys were anesthetized and laser beams shone into their eyes in order to determine the damage threshold for various beam intensities and wavelengths. The primates were then later “sacrificed” and their eyes dissected to obtain the microphotographs showing possible radiation damage. This is clearly not the sort of research that can be conducted on human subjects.
In their paper, the authors reported the following radiation damage thresholds for a 441.6 nm helium-cadmium laser:
| 1 second | 16 seconds | 100 seconds | 1000 seconds |
| 0.91 watts / cm2 | 0.41 watts / cm2 | 0.20 watts / cm2 | 0.03 watts / cm2 |
(A joule is one watt-second, so 0.03 watts per square centimeter for 1,000 seconds is 30 joules/cm2, as indicated in Figure 3 above.)
In their 1978 paper, the authors replaced the laser beam with a 2,500-watt xenon lamp and a 6 nm bandwidth interference filter at 441 nm with associated optics to focus the beam onto a 1-mm diameter region of the monkey’s retina for up to 1,000 seconds. (Kids, don’t try this science experiment at home …)
Grim and disturbing details aside, we have finally answered the question – where did the information quoted by Kitchel and through her by Willmorth come from?
What we have not answered however is the question of whether this research is relevant to the “blue light hazard” issue.
Inadmissible Evidence
It is true that Ham et al. (1976, 1978) established that exposure to blue light can cause retinal lesions, however microscopic. However, maximum exposure times of 1,000 seconds (16 minutes) are hardly “long-term exposure” as described by Willmorth (2014). Simply put, the research of Ham et al. did not address the issue of long-term exposure to blue light.
Equally interesting is this quote: (Ham et al. 1976):
“… the solar retinal irradiance at 440 nm for a 20-nm spectral band is approximately 0.20 W/cm2 at midday for an eye gazing directly at the Sun at sea level for a 2-mm diameter pupil. In comparison, the threshold irradiance for a 100-sec exposure to the 441-nm laser line of He-Cd is 0.20 W/cm2. Thus, sungazing at bright midnoon for 100 sec can produce a threshold lesion … those subject to exposure to bright sunlight over long periods should take precautions to shield their eyes from the short wavelengths of solar radiation.”
In other words, what Ham et al. discovered through careful experiment was the glaringly obvious: do not stare at the noonday sun without blinking for longer than fifteen minutes. This is not mockery of their research – Ham et al. were investigating the distinction between thermal and photochemical effects of high-intensity light on the retina. Their comparison with sungazing, while instructive, was merely by way of analogy to put the beam intensity levels into context for the reader.
This is not to say that long-term chronic exposure to blue-rich light does not result in adverse health effects, including cataracts and age-related macular degeneration. Ham et al. did their work nearly forty years ago. There may well be more recent research that is relevant to the “blue light hazard,” such as for example Shang et al. (2014). (Whether this fundamentally flawed paper is applicable to human vision is a separate issue.)
Regardless, the research of Ham et al. is “inadmissible evidence” (to use the legal expression) with respect to the long-term effects of blue light exposure. It is not a question as to whether it is right or wrong, but simply that it does not apply.
The problem – the real problem – is that journalists are expected to interpret academic research for the general public. Like Willmott and Kitchel, they may have considerable knowledge in their fields of expertise. Unfortunately, the “blue light hazard” issue intersects research fields in both lighting and medicine. As such, journalists need to take particular care in interpreting published papers on the topic. For whatever reason, there was some miscommunication in this case.
Conclusion
To summarize, there may possibly be persuasive evidence that long-term chronic exposure to blue-rich (i.e., high CCT) lighting may adversely affect our vision and health. Articles such as “The Dark Side of BLUE LIGHT” (Willmorth 2014a) and “The Effects of Blue Light on Ocular Health” (Kitchel 2000) have referred to the academic research literature (Ham et al. 1980) as evidence of danger. Unfortunately, all that this research proved in the context of the “blue light hazard” was the obvious: do not stare at the noonday sun without blinking for longer than fifteen minutes.
As Kevin Willmorth said, “… there is a need for more focused research leading to practical recommendations on this subject.” In the meantime however, this author at least is still looking for persuasive evidence that there is any significant blue light hazard associated with high-CCT LED lighting.
At the same time, I agree with Kevin when he says (Willmorth 2014b), “I cannot recommend [that] anyone apply poor-quality, low color performance light sources of any type when alternative are available” … but this is just our opinion. In the absence of evidence to the contrary, there does not appear to be any scientific reason to be concerned about blue-rich lighting in typical interior environments.
UPDATE – November 8, 2014
In 2010, the French Agency for Food, Environmental and Occupational Health & Safety (ANSES) published a 310-page report (in French) titled, “Health Effects of Lighting Systems Using Light-Emitting Diodes (LEDs)” (ANSES 2010), with an English-language opinion and summary (ANSES 2010b). Page 3 of the summary reads:
“Some scientific studies [Dawson et al., 2001, Ueda et al., 2009], based on laboratory experiments with blue LEDs conducted on monkeys, give reason to suspect a danger for the retina related to exposure to light-emitting diodes.”
Déjà vu, non?
The remainder of the summary offers recommendations that are reasonable in view of the photobiological risks of high-brightness LEDs. However, the risk of having the “reason to suspect” statement taken out of context in support of the “blue light hazard” meme remains.
Reading the referenced papers of course provides more information. Dawson et al. (2001) sacrificed five rhesus monkeys after exposing them to between 5 and 54 joules/cm2 of blue light from a 458 nm argon laser. Again, this is roughly equivalent to staring at the noonday sun without blinking for 3 to 25 minutes.
Ueda et al. (2009) sacrificed eight monkeys (two rhesus and six long-tailed macaque) after exposing them to between 20 and 60 joules/cm2 from Nichia NSPB550S blue LEDs with a dominant wavelength of 465 nm. Similar to the earlier studies of Hall et al. (1976), they reported retinal lesions after exposure to 35 joules/cm2, but no detectable results after exposure to 20 joules/cm2.

There must be something apparently irresistible about such studies, as van Norren et al. (2011) provide a critical review of no fewer than 56 papers on the topic. What is interesting is that the results of eight such experiments (including Ham et al. 1976) yielded essentially the same results for rabbits and monkeys:
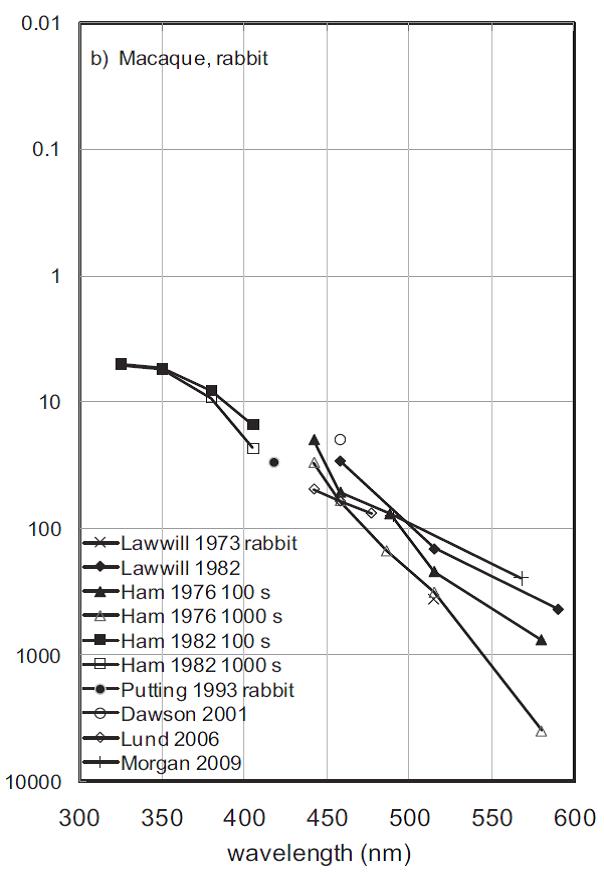
while the results for rodents (including both albino and pigmented rats) were equally similar. To summarize these results, do not stare at the noonday sun without blinking for longer than fifteen minutes. Once again, the evidence that long-term chronic exposure to blue-rich (i.e., high CCT) lighting may adversely affect our vision and health is not persuasive.
A much more interesting publication was recently published by the International Energy Agency (IEA 2014). Providing a wealth of information on the photobiological hazards of solid-state lighting, it concludes in Section 5.6.3, Potential Effects of Long-term Exposures, that:
“The ICNIRP exposure limit values do not take into account the possibility of an exposure over an entire lifetime. Very little is known about the effects of life‐long cumulated exposures to blue light emitted by LEDs. According to the Scientific Committee on Emerging and Newly Identified Health risks (SCENIHR) of the European Commission [SCENIHR 2012], no evidence was found indicating that blue light from artificial lighting belonging to Risk Group 0 would have any impact on the retina graver than that of sunlight. The SCENIHR states that IEC 62471 gives limits that are protective against acute effects, while long‐term effects are only marginally considered and estimated to be of negligible or small risk.”
Following the paper trail to its end, we have (SCENIHR 2012):
“Evidence from in vitro experiments suggest that blue light at 10 W/m2 induces photochemical retinal damages (Class II) up on acute (hours) exposure, and animal experiments and in vitro studies suggest that cumulative blue light exposure below the levels causing acute effects also can induce photochemical retinal damage.
“There is no consistent evidence from epidemiological studies regarding the effect of long-term exposure to sunlight (specifically the blue component of sunlight) and photochemical damage to the retina (particularly to the retinal pigment epithelium), which may contribute to age-related macular degeneration (AMD) later in life. Whether exposure from artificial light could have effects related to AMD is uncertain.
“There is no evidence that artificial light from lamps belonging to RG0 or RG1 would cause any acute damage to the human eye. Studies dedicated to investigating whether retinal lesions can be induced by artificial light during normal lighting conditions are not available. Lamp types belonging to RG2 and higher are usually meant to be used by professionals in locations where they do not pose a risk. Chronic exposure to blue light from improperly used lamps could, in theory, induce photochemical retinal damage in certain circumstances. There is however no evidence that this constitutes a risk in practice. It is unlikely that chronic exposures to artificial light during normal lighting conditions could induce damage to the cornea, conjunctiva or lens.”
and finally from the abstract (ibid):
“There is no evidence that blue light from artificial lighting belonging to Risk Group 0 (“exempt from risk”) would have any impact on the retina graver than that of sunlight. Blue light from improperly used lamps belonging to Risk Groups 1, 2, or 3 could, in theory, induce photochemical retinal. There is no evidence that this constitutes a risk in practice. Other damages to the eye from chronic artificial light exposure during normal lighting conditions are unlikely. Exposure to light at night (independent of lighting technology) while awake (e.g. shift work) may be associated with an increased risk of breast cancer and also cause sleep, gastrointestinal, mood and cardiovascular disorders.”
In the end, we have no option but to appeal to authority (argumentum ab auctoritate). SCENIHR (2012) represents the opinions of a dozen medical professionals who are presumed experts in the field. The difference however is that they are specifically addressing the issue of “blue light hazard” with full knowledge (circa 2012) of existing lighting technologies. Their 118-page report includes a staggering 341 references to the academic literature.
[UPDATE 14/12/11: The Global Lighting Association, representing ten regional lighting industry associations from around the world, released a white paper in March 2012 with the abbreviated title “Optical Safety of LEDs.” There are two versions, one being a 22-page document with a detailed and indepth analysis of the photobiological risks of common “white light” lamp types, and the other being a 4- page abridged document. Their well-documented position statement is simple: “… based on accepted and widely adopted safety standards for lamps, is that all general lighting sources, including LED and CFL sources (either lamps or systems) and luminaires, can be safely used by the consumer when used as intended.”] There may be medical studies yet to be conducted that will demonstrate a blue light hazard for solid-state lighting in typical interior lighting applications. However, the absence of such evidence to date is highly persuasive: there is no scientific reason to be concerned about blue-rich lighting in typical interior environments.
References
ANSES. 2010a. Effets sanitaires des systèmes d’éclairage utilisant des diodes électroluminescentes (LED). Maisons-Alfort, France: French Agency for Food, Environmental and Occupational Health & Safety.
ANSES. 2010b. Opinion of the French Agency for Food, Environmental and Occupational Health & Safety in response to the internally-solicited request entitled “Health Effects of Lighting Systems Using Light-Emitting Diodes (LEDs).” Maisons-Alfort, France: French Agency for Food, Environmental and Occupational Health & Safety.
Berman, S., M. Navvab, M. J. Martin, and J. Sheedy. 2006. “A Comparison of Traditional and High Color Temperature Lighting on the Near Acuity of Elementary School Children,” Lighting Research & Technology 38(1):41-52.
Berman, S., and R. Clear. 2013. “Another Blue Light Hazard?,” Lighting Design & Application 43(3):65-68.
Bullough, J. D. 2000. “The Blue-Light Hazard: A Review,” Journal of the Illuminating Engineering Society 29(2):6-14.
Dawson, W., T. Nakanishi-Ueda, D. Armstrong, D. Reitze, D. Samuelson, M. Hope, S. Fukuda, M. Matsuishi, T. Ozawa, T. Ueda and R. Koide. 2001. “Local Fundus Response to Blue (LED and Laser) and Infrared (LED and Laser) Sources,” Experimental. Eye Research 73:137-147.
GLA. 2012. Optical and Photobiological Safety of LED, CFLs, and Other High Efficiency General Lighting Sources. Global Lighting Association.
Ham, W. T., Jr., and D. H. Sliney. 1976. “Retinal Sensitivity to Damage from Short Wavelength Light,” Nature 260:153-154.
Ham, W. T., Jr., J. J. Ruffolo Jr., H. A. Mueller. A. M. Clarke, and M. E. Moon. 1978. “Histologic Analysis of Photochemical Lesions Produced in Rhesus Retina by Short-wave-length Light,” Investigative Ophthalmology & Visual Science 17(10):1029-1035.
Ham, W. T., Jr., H. A. Mueller, J. J. Ruffolo Jr., and D. Guerry. 1980. “The Nature of Retinal Radiation Damage: Dependence on Wavelength, Power Level, and Exposure Time,” Vision Research 20(12):1105-1111.
Holzman, D. C. 2010. “What’s in a Color? The Unique Human Health Benefits of Blue Light,” Environmental Health Perspectives 118(1):A22-A27.
IEA. 2014. Energy Efficient End-Use Equipment (4E) Solid State Lighting Annex – Potential Health Issues of Solid State Lighting Final Report. Paris, France: International Energy Agency.
Kitchel, E. 2000. “The Effects of Blue Light on Ocular Health,” Journal of Visual Impairment and Blindness 94(6):399-403.
SCENIHR. 2010. Health Effects of Artificial Light. Brussels, Belgium: European Commission (Scientific Committee on Emerging and Newly Identified Health Risks).
Shang, Y.-M., G.-S. Wang, D. Sliney, C.-H. Yang, and L.-L. Lee. 2014. “White Light-Emitting Diodes (LEDs) at Domestic Lighting Levels and Retinal Injury in a Rat Model,” Environmental Health Perspectives 122(3):269-276.
Ueda, T., T. Nakanishi-Ueda, H. Yasuhara, R. Koide, and W. W. Dawson. 2011. “Eye Damage Control by Reduced Blue Illumination,” Experimental Eye Research 89:863-868.
van Norren, D., and T. G. M. F. Gorgels. 2011. “The Action Spectrum of Photochemical Damage to the Retina: A Review of Monochromatic Threshold Data,” Photochemistry and Photobiology 87:747-753.
Willmorth, K. 2014a. “The Dark Side of BLUE LIGHT,” Architectural SSL 05.14, pp. 12-16.
Willmorth, K. 2014b. Personal communication.
0 Comments